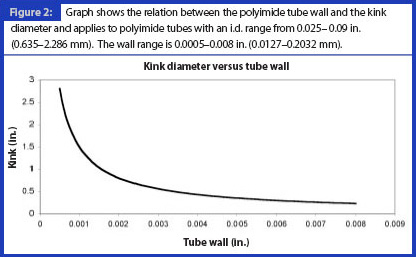
As a class of organic resins, polyimides exhibit outstanding engineering properties, especially thermal stability, dielectric strength, mechanical strength, temperature stability and chemical resistance, see Table I. Although polyimide resin structures were known about in the 1950s, it was the introduction of polyimides in the 1960s that made significant contributions to meeting exacting industry demands. In 1961 DuPont introduced film (under the trade name Kapton) and varnishes for electrical applications and wire insulation. Subsequently moulding powders, laminating resins, foams and composite materials and high performance adhesives became available.1
Seamless polyimide tubing was discovered in the 1970s. Previously, only spiral wound tubing made from Kapton film had been available. Spiral wound tubing does not provide the properties or the dimensions of the seamless design. Seamless polyimide tubing was introduced to the catheter market in the early 1980s.1 One of the most commonly asked questions in the catheter design market is, “how thin can the wall be made?” The limiting factor in making thin walled polyimide tubing for medical applications is having sufficient tube integrity to allow the tube to be removed from the mandrel on which it is made. A polyimide tube can be made with a wall thickness of less than 0.0005 in. (0.0127 mm), but removing that tubing from the mandrel can prove to be a real challenge. Handling a thin walled tube of this size can also test traditional material handling methods.
Comparing thermosets and thermoplastics
Polyimide is considered to be a thermoset polymer, and once cured, it cannot be reflowed or melted. Thermosetting polymers (thermosets) cure to a stronger form through the addition of energy. The energy used to cure the thermoset may be in the form of heat, chemical reaction or irradiation. Thermoset materials are usually liquid or malleable prior to curing. They are typically strong materials because their molecular structural units are held together by strong, covalent chemical bonds. In these materials, the resin is transformed into plastic by cross linking. The cross linking process forms a molecule with a larger molecular weight, which results in a material with a higher melting point than the surrounding ambient temperature. Subsequent reheating of the material results in it reaching its decomposition temperature before the melting point is obtained. A thermoset material cannot, therefore, be melted; it simply decomposes.
Thermoplastic polymers are normally produced in one step and then made into products in a subsequent process. Thermoplastics are materials that melt into a liquid when heated and solidify when cooled sufficiently. Typically, the bonding forces within thermoplastics tend to be weaker than bonds within thermosets. An example of a thermo-plastic polymer is polyether block amide (trade name Pebax). Thermoplastic polymers differ from thermosetting polymers because they can be remelted and remoulded.
Thermosetting polyimides are commercially available in many uncured forms, including stock shapes, thin sheets, laminates and machined parts. Polyimides are thermoset when cured and are made to be strong, stable at high temperatures and chemically inert. In addition, polyimide is chemically resistant to almost everything except extremely strong alkalines such as potassium hydroxide or sodium hydroxide.
In the general medical design market place, polyimide and polyimide tubing are not well understood. Any material that is not well understood is a material for which many myths develop over time.
Myth 1: Polyimide tubing is difficult to bond
Polyimide tubing is constructed in many layers on a mandrel; the process is known as “dipping” or “dip dispersion” in which each layer is applied and cured until the desired thickness is achieved. Each layer of the tube is extremely thin: in the order of 0.00010–0.00012 in. (0.00254–0.00305 mm) in thickness. Each liquid layer is put through a series of three temperature changes. The first temperature zone is the temperature at which the solvent evaporates from the layer. In the second temperature zone, catalysts are activated in the polymer to prepare it for cross linking. The final and hottest temperature zone is used to crosslink that layer to the layer beneath it.
This cross linking is the step that thermosets the polyimide. The outer surface of a polyimide tube, because it is formed directly from liquid, has a glass-like surface without imperfection. There are no waves, no die marks and no pinholes present. There is nothing that will mechanically assist in bonding. Depending on the particular application, some surface preparation may improve bondability. Surface preparation can come in many forms. It can be as simple as roughening the surface with abrasive materials such emery cloth or sandpaper, or it can be as sophisticated as corona or plasma treatment.
Because polyimide is a thermoset plastic, it does not melt. Ultrasonic welding, solvent bonding and other thermal bonding techniques will not yield tremendous results. From experience, the most successful adhesives for bonding to polyimide are cyanoacrylates and two-part epoxies. Design engineers should refer to a reputable adhesive company for guidance on the appropriate adhesive for an application. One thing is certain: attempting to UV cure through polyimide is a futile effort; polyimide absorbs the vast majority of the ultraviolet radiation that is employed, leaving the adhesive uncured. Bonding to polyimide can be successful and easy when a little thought is put into the process in advance.
Myth 2: Polyimide tubing kinks too easily
Every plastic tube kinks at some point and material selection is a matter of engineering tradeoffs. Polyimide has good mechanical properties (Table I), but it does not have magical qualities. Catheter design has become complex during the past few years and engineers rarely want a tube that has the same properties at both ends of the tube.
When the ratio of the tube diameter to wall thickness is, in relative terms, small, a tube can be bent to a small diameter without kinking. As the tube diameter increases and as the wall thickness decreases, the extent (diameter) to which the tube can bend without kinking decreases/shrinks. As a tube bends, the cross-section of the tube in the bend becomes increasingly oval until the point at which the tube finally kinks. The stronger the plastic, the less the material is able to stretch on the outside of the bend or compress on the inside of the bend. Thus, stronger plastics do tend to kink more easily at a larger radius for a given set of dimensions. The dimensions and material strength are the critical operating parameters in this equation (see Figures 1 and 2).
A tube made from polyimide with an inside diameter of 0.040 in. (1.016 mm) and a wall thickness of 0.00075 in. (0.01905 mm) will kink more easily at a larger radius than a similar sized tube made from a soft thermoplastic polymer such as Pebax. However, the polyimide tube is significantly stronger and a soft Pebax tube in those dimensions is difficult to obtain.
Taking material strength into consideration is essential when considering kink radius. Reinforcement can also be added. A coil reinforcement made from stainless steel can be placed within the wall of a polyimide tube to help spread the bend over a distance and to prevent the tube from becoming as oval in the bend area. Reinforcement in the form of a coil can significantly improve kink results while maintaining tube strength and dimensions.
Myth 3: Polyimide tubing is not very flexible
According to Webster’s dictionary, flexible means capable of being bent or flexed. Polyimide tubing can be bent and flexed. However, it may require more force to bend a polyimide tube than a softer plastic. This fact works both for and against polyimide as a material in catheter design. Polyimide is not the perfect material for every application, but when superior strength is required, polyimide should be a critical component of the design.
More recently, improved manufacturing methods are allowing the use of composite materials. In many of today’s catheter designs, polyimide can be a critical strengthening component within the overall device. Composite material ideas may include:
- fluoropolymer polytetrafluoroethylene (PTFE) or fluorinated ethylene propylene liners
- braid, coil or axial reinforcement
- single or multi-durometer outer layers
- a-traumatic tips with or without marker bands
- laser ablation
For strength, especially in tight places, polyimide is the recommended material.
Myth 4: Polyimide tubing is brittle
If polyimide tubing is properly cured, it is not easily broken, cracked or snapped, in other words, it is not brittle. However, an extremely thin layer of polyimide placed over a braid can be punctured by the braid if the tube is kinked. Caution should be exercised when employing extremely thin walled, braided, polyimide tubes. On a pure polyimide tube, in excess of 85% of the original material properties of the tube can be regained after kinking by simply heating the tube to 200 ºC to stress relieve the affected area. If polyimide tubing is found to be brittle, it has not been properly cured and should be discarded.
Polyimide tubing is produced in many layers. Although those layers are molecularly bonded to the layers both above and below, excessive shear stress applied to the wall of a polyimide tube can overcome the covalent bond strength and cause delamination. Reputable manufacturers of polyimide tubing implement controls and testing in their operations to ensure proper cross linking of layers to guard against delamination.
Myth 5: Polyimide tubing is difficult to drill, machine and form
Although polyimide tubing is a thermoset material, a limited amount of forming using techniques such as flaring and/or tapering can be performed. In general, forming is done at relatively high temperatures utilising mandrels to support every aspect of the process.
Traditionally, punches have been used to create holes in catheter surfaces. More recently, laser ablation has proven to be extremely effective for a variety of catheter features, including holes, slots, chamfers, outer diameter reduction, end cuts and printing. Laser ablation accomplishes all that the mechanical methods of the past achieved without leaving any burrs and without imparting any excessive stress to the part.
Myth 6: Polyimide tubing has a high coefficient of friction
Because the surface of a polyimide tube is produced by curing a liquid, the surface is perfectly smooth. When an extremely smooth surface comes into direct contact with another smooth material there is a great deal of contact area that may lead to friction. The actual coefficient of friction (COF) of polyimide is 0.50 compared with PTFE, which has a COF of 0.10–0.20. To combat the difference in frictional indices, many manufacturers of polyimide tubing have created composite materials to reduce surface friction. These coatings generally reduce the COF to a more manageable value of approximately 0.30–0.35. In some cases, pure PTFE liners can be employed to reduce friction to even lower levels.
The choice for the future
Polyimide tubing has been a resource in the catheter design engineer’s toolbox for more than 25 years, but despite its obvious strengths, relatively little is known about how best to utilise it. There are some challenges with this material, as with any material. The primary benefit of polyimide tubing is its strength-per-unit-size. The medical device industry, in an effort to reduce the total cost of health care, is attempting to treat patients less invasively by placing devices that are able to accomplish more in smaller and smaller pathways. With a little thought and ingenuity, polyimide will allow design engineers to fulfill their device needs for years to come.
Reference
1. Polyimides: Fundamentals and Applications, M.K. Ghosh, K.L. Mittal, Eds., Marcel Dekker, New York, New York, USA (1996).
Timothy J. Lynch is Operations Manager at MicroLumen Inc., 7624 Bald Cypress Place, Tampa, Florida 33614, USA, tel. +1 813 886 1200, e-mail: tlynch@microlumen.com, www.microlumen.com.
This article was published in MDT May/June 2008
